Open Access
Open Access Abstract
Colonic lipomas are benign tumors resulting from the proliferation of mature fat cells. Gastrointestinal lipomas are rare, often asymptomatic, and most are detected through diagnostic imaging devices such as colonoscopy and abdominal-pelvic computed tomography. Lipomas of the colon were first reported by Bauer in 1757 and are most often located in the ascending colon near cecum. Approximately 90% of colonic lipomas are located in the submucosa. The remainder of these tumors is intramucosal in origin. The reported incidence of colonic lipoma ranges from 0,2% to 4,4%. These fatty tumors are rarely greater than 2 cm in size and are rarely symptomatic. Lipomas that grow more than 4 cm in size can lead to obstruction and intussusception requiring surgical or endoscopic resection. Colonic lipomas may be challenging to diagnose as they may be asymptomatic for a long time or misdiagnosed as other's conditions. Atypical etiologies of intestinal obstruction should be considered in patients with persistent intermittent abdominal discomfort. Even though benign, some abdominal tumor conditions may be presented as cases of emergency care. Symptomatic colonic lipomas can be managed by endoscopy or surgery. Polypectomy through endoscopy is the treatment choice for lipomas considered of low complication risk. These are lipomas with less than 2 cm diameter or pedunculated lipomas with a thin tail. When greater than 2 cm, surgery represents the standard therapeutic option for lipomas. In this report, we present two cases of symptomatic colonic lipomas: one case of splenic flexure lipoma and one case of lipoma in the sigmoid colon. Both cases have been noted with intestinal obstruction. Those two patients performed laparoscopic colectomy. The operation and post-operative recovery were satisfactory. Both of the patients were discharged after taking seven days of post-operative care. Through this article, we would like to introduce the incidence, clinical features, diagnostic facilities, and surgical treatment of this benign tumor.
INTRODUCTION
Colonic lipomas are benign tumors resulting from the proliferation of mature fat cells. Gastrointestinal lipomas are rare and often asymptomatic, and most are detected through diagnostic imaging devices such as colonoscopy and abdominal-pelvic computed tomography. Lipomas of the colon were first reported by Bauer in 1757 and are most often located in the ascending colon near the cecum. Approximately 90% of colonic lipomas are located in the submucosa; the remainder of these tumors are submucosal or intramucosal in origin. The reported incidence of colonic lipoma ranges from 0,2% to 4,4% 1 . These fatty tumors are rarely greater than 2 cm in size and rarely cause symptoms. Colonic lipoma larger than 4cm in size may cause obstruction and intussusception in one or more parts of the large intestine 2 .
CASE REPORTS
Case number 1
A female patient, 55 years old, was admitted to the hospital because of left upper quadrant abdominal pain lasting one week. The patient had intermittent cramping pain, each episode lasting for 30 seconds. Pain increases with bowel movements. No vomiting, no fever. The conditions at admission were recorded: her pulse was 80 times/minute, the temperature was 37 o C, her blood pressure was 120/80 mmHg, respiratory rate was 16 times/minute. The abdominal examination noted mild pain in the left upper quadrant, and there was a mobile mass in the left hypochondrium, soft density. An anorectal investigation revealed no abnormalities.
Abdominal ultrasound results showed a thick echo structure, heterogeneous, well-defined, 55x37 mm, and no angiogenesis in the descending colon. No bowel obstruction was seen on ultrasound. Blood tests showed no infection or anemia.
The computed tomography results showed that there was a 4x5x6cm tumor at the splenic flexure colon. Colonoscopy results showed a lipoma-like tumor on the macroscopic image, about 35cm from the anal border.
The patient was diagnosed with semi-obstruction due to a descending colon tumor and was scheduled for elective laparoscopic left colectomy. The patient was lying supine, with the head tilted to the right, under endotracheal anesthesia. The surgical team carried it out into the abdomen with four trocars. Examination of the abdomen noted that the abdomen was clean, and the liver was pink and smooth. The loops of the small intestine are not dilated. The colon is slightly dilated. Exploration revealed that the splenic flexure colon had a 5x6 cm intussusception, with a tumor inside. Density was soft, mimicking colonic polyp causing intussusception. No mesenteric lymph nodes were seen. The lower part of the colon collapses. Other organs have not reported any abnormalities. The surgical team performed a left colectomy containing the tumor, connecting the transverse colon - sigmoid colon laterally. The colonic lipoma was then revealed at the size of 3x4x3 cm ( Figure 1 ).
Postoperatively, the patient recovered well and had a good bowel movement on the 3rd postoperative day. After surgery, there was no abdominal fluid by ultrasound examination. Blood tests showed no abnormality. The patient was discharged on postoperative day 7. The postoperative pathology results showed lipoma.
Figure 1 . Lipoma of splenic flexure colon after bisection (Source: Binh Dan hospital)
Case number 2
A female patient, 63 years old, was admitted to the hospital because of abdominal cramping pain for less than two weeks. Pain increases with bowel movements. No fever, no vomiting recorded. The condition at admission: her pulse was 75 times/minute, her temperature was 37 o C, her blood pressure was 140/80 mmHg, respiratory rate was 20 times/minute. Abdominal examination revealed mild pain in the lower right quadrant. An anorectal investigation revealed no abnormalities.
Blood tests revealed no infection or anemia. Cancer markers (CEA, CA 19-9) were not increased. Endoscopic results showed a sigmoid colon tumor, 20cm from the anal border, large in size, occupying the entire colon. Ultrasound showed a 6x4cm thick echogenic mass behind the bladder. No intussusception was recorded on ultrasound. The results of a large computed tomography scan showed an image of intussusception in the sigmoid colon due to a fatty tumor.
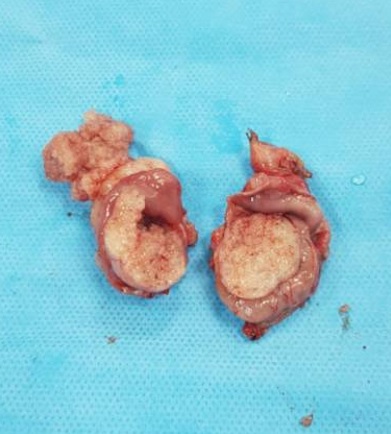
The patient was scheduled for laparoscopic sigmoidectomy. The team operated on the abdomen with four trocars. Intra-abdominal exploration revealed that the terminal sigmoid colon had a tumor size of 5x5x4cm ( Figure 2 , Figure 3 ), no invasion of the lymph nodes, and no adhesions to adjacent structures: liver pink, smooth surface. The peritoneum does not metastasize. The upper colon is dilated, with signs of semi-obstruction. The small intestine is not dilated. The surgical team carried out sigmoid colon closure, end-to-end anastomosis.
Postoperatively, the patient recovered well and passed bowel movements on postoperative day 1. After surgery, the patient was examined by ultrasound, and no abdominal fluid was noted. Postoperative blood tests did not reveal infection or anemia. Pathology resulted in a lipoma ( Figure 4 ). The patient was discharged on postoperative day 7.
Figure 2 . Sigmoid lipoma before and after bisection (Source: Binh Dan hospital).

DISCUSSION
Presentation and diagnosis
In most cases, colonic lipoma causes no symptoms and may just be found by colonoscopy or operation for other reasons. The size of colonic lipoma is strongly related to a patient's symptoms. Around 75% of patients with lipomas bigger than 4cm in diameter may have symptoms from mild (abdominal pain, increased bowel movement) to severe (intestinal obstruction, gastrointestinal bleeding). 3 , 4 . Colonic lipomas are mostly benign, with only about 6% causing symptoms. Common symptoms of colonic lipoma are gastrointestinal bleeding (54.5%), abdominal pain (42.4%), change in bowel habits (24.2%). Other rare symptoms include intestinal perforation, intussusception, and rectal prolapse 5 , 6 , 7 . However, some have larger colonic lipoma but have no symptoms at all. Those situations delay the making of diagnosis and, therefore, may increase the patients' risk. Furthermore, colonic lipomas may mimic colonic cancer in presentation due to the similarities in age and symptoms 8 .
Since it is quite difficult to diagnose colonic lipoma clinically, tools such as radiographic, endoscopic, ultrasound, magnetic resonance imaging (MRI), and postoperative pathology are important in making the absolute diagnosis. Endoscopic ultrasound (EUS) generally illustrates a hyperechoic (or hypoechoic in some cases) lesion from the submucosal layer 9 . Colonic endoscopic and biopsy are also important to diagnose non-emergency patients. However, sometimes even experienced endoscopists mistake a colonic lipoma with colorectal cancer 10 . When complications appear, such as obstruction, torsion, and ischemia…, abdominal ultrasound can quickly assess the patient's problem and point out the emergency situation.
The histopathologic analysis is the most important tool for making a definitive diagnosis and is often made after surgeries or endoscopic biopsy. The final diagnosis of lipoma is based on histopathological findings. Most histopathological findings show well-differentiated lipomas, possibly with surrounding inflammatory tissue. In some cases, microscopic results show a pseudosarcoma. In general, patients with colonic lipoma have a good prognosis. The rate of malignancy of colon lipoma has not yet been recorded 1 .
Computer tomography (CT) and MRI are also used to access one with colonic neoplasm. Because of characteristics for fatty tissue, they can illustrate colonic lipomas and the position, adjacent lesions, or complications. But just like colonic endoscopy, CT or MRI may mistake a large tumor with other kinds of colonic neoplasms. Therefore, they are not used to confirm the problem 11 .
Figure 3 . Intussusception in the sigmoid colon due to a fatty tumor (Source: Binh Dan hospital)

Management
There are many treatments for colonic lipomas. Endoscopic resection can be performed for tumors less than 2 cm in size. However, for tumors larger than 2 cm, endoscopic resection increases the risk of colonic perforation because lipomas contain more water, so endoscopic electrocoagulation will be less effective 12 . Colectomy containing lipoma is usually indicated when: 1) tumor size is larger than 2 cm; 2) the preoperative diagnosis is unknown; 3) symptomatic lipoma; 4) lipoma invades muscle or serosa; 5) lipomas that are not resectable through gastrointestinal endoscopy 1 .
Before, they believed that endoscopic resection was related to a higher risk of perforation and bleeding, but recent studies have shown brighter results as the complication rates are acceptable 13 , 14 . When the tumors are large enough to make it difficult for endoscopic resection, or the situations turn worse, such as intussusception or intestinal obstruction, surgical resection is the treatment of choice. Besides, surgery is also the first choice for sessile lipomas and has limited depuncles 8 . There are surgical techniques that can be used, such as hemicolectomy, segmental resection, or local excision, depending on the site and size of the tumor 8 , 6 , 15 . In their case study, Gould and colleagues used surgical resection of the colonic segment of intussusception. Later histopathology, the mass was found to be colonic lipoma 16 .
Figure 4 . Microscopic slides revealing mature fat cells (Source: Binh Dan hospital)

CONCLUSION
Colon lipoma is a relatively rare disease in benign tumors of the gastrointestinal tract. Typically, colonic lipomas are minor and cause no symptoms. Symptoms usually appear when the cancer is more significant than 2cm, in which bowel obstruction and bleeding are common. Currently, laparoscopic resection of the colon containing the tumor is still effective in treating complications of this tumor.
CONSENT
Written informed consent was obtained from our patient for publication of this case report and any accompanying images.
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interests.
AUTHORS’ CONTRIBUTION
Phu V. Pham had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design : Phu V. Pham, Huu P. Nguyen.
Drafting of the manuscript : Phu V. Pham, Huu P. Nguyen, An K. Vu
Supervision : Hung V. Tran.
References
- Paik Hyun June, Yu Hyeon. Giant lipoma in the splenic flexure causing colonic intussusception. Journal of Minimally Invasive Surgery. . 2012;:143-148. Google Scholar
- Daniel L. Gould, C. Anne Morrison, Kathleen R. Liscum, Eric J. Silberfein. A Lipoma of the Transverse Colon Causing Intermittent Obstruction: A Rare Cause for Surgical Intervention. Clinical case studies. . 2011;:487-490. Google Scholar
- Bahadursingh AM, Robbins PL, Longo WE. Giant submucosal sigmoid colon lipoma. Am J Surg. . 2003;(186):81-82. Google Scholar
- Rogy MA, Mirza D, Berlakovich G, Winkelbauer F, Rauhs R. Submucous large-bowel lipomas-presentation and management. An 18-year study. Eur J Surg. . 1991;(157):51-55. Google Scholar
- Franc‑Law JM, Bégin LR, Vasilevsky CA, Gordon PH. The dramatic presentation of colonic lipomata: Report of two cases and review of the literature. Am Surg. . 2001;(67):49-4. Google Scholar
- Ghidirim G, Mishin I, Gutsu E, Gagauz I, Danch A, Russu S. Giant submucosal lipoma of the cecum: report of a case and review of literature. Rom J Gastroenterol. . 2005;(14):393-396. Google Scholar
- Buetow PC, Buck JL, Carr NJ, Pantongrag‑Brown L, Ros PR, Cruess DF. Intussuscepted colonic lipomas: Loss of fat attenuation on CT with pathologic correlation in 10 cases. Abdom Imaging. . 1996;(21):153-156. PubMed Google Scholar
- Geetha N, Gouglas G. Adler. Review large colonic lipomas. Gastroenterology & Hepatology. . 2011;(7):490-492. Google Scholar
- Shepherd BD, Merchant N, Fasig J, Schwartz DA. Endoscopic ultrasound diagnosis of pelvic lipoma causing neurologic symptoms. Dig Dis Sci. . 2006;(51):1364-1366. PubMed Google Scholar
- Martin P, Sklow B, Adler DG. Large colonic lipoma mimicking colon cancer and causing colonic intussusception. Dig Dis Sci. . 2008;(53):2826-2827. PubMed Google Scholar
- Liessi G, Pavanello M, Cesari S, Dell'Antonio C, Avventi P. Large lipomas of the colon: CT and MR findings in three symptomatic cases. Abdom Imaging. . 1996;(21):150-152. PubMed Google Scholar
- Hsu-Heng Yen. Colonic lipoma. Video Journal and Encyclopedia of GI Endoscopy. . 2013;(1):661-662. Google Scholar
- Pfeil SA, Weaver MG, Abdul-Karim FW, Yang P. Colonic lipomas: outcome of endoscopic removal. Gastrointest Endosc. . 1990;(36):435-438. Google Scholar
- Yu HG, Ding YM, Tan S, Luo HS, Yu JP. A safe and efficient strategy for endoscopic resection of large, gastrointestinal lipoma. Surg Endosc. . 2007;(21):265-269. PubMed Google Scholar
- Jiang L, Jiang LS, Li FY, et al. Giant submucosal lipoma located in the descending colon: a case report and review of the literature. World J Gastroenterol. . 2007;(13):5664-5667. Google Scholar
- Gould DJ, Morrison CA, Liscum KR, Silberfein EJ. A lipoma of the transverse colon causing intermittent obstruction: a rare cause for surgical intervention. Gastroenterol Hepatol (N Y). . 2011;(7):487-490. Google Scholar